I guess someone published this again, since the Walkerton outbreak of E. coli O157 which killed seven and sickened over 2,000 k in a town of 5,000 happened in May 2000.
I know it’s not the best writing, but I tried, and it was 20 years ago. I severed on an expert (I hate that word) committee and we wrote our report.
We live near the publicaly funded Princess Alexandria hospital in Brisbane.
A helicopter flies over our house a couple of times a day bringing some victim from the outback or the coast.
The state of Queensland is really, really big.
It reminds me of my Walkerton-resident friend and what he went through in the aftermath of the E. coli O157 outbreak in drinking water.dying being flown to the medical center in London, Ontario (that’s in Canada, like Walkerton).
I think of Jim and the victims every time a chopper goes past.
The E. coli O157:H7 waterborne outbreak in Walkerton, Ont., Canada, in May 2000, presented a clear and present danger of risk to citizens who consumed that water — at least in retrospect. More challenging though, is to know when a risk is severe enough to warrant extraordinary communications and how best to compel citizens to comply with health advisories.
Risk theory, involving assessment, management and communication, is important to underpin discussions of how regulators, industry and citizensincorporate and act on information about risks — such as the hazards posed by E. coli O157:H7 in drinking water. Today it is well accepted that the three components of risk analysis cannot be separated and are, in fact, integrated, and that communication involves the multi-directional flow of information.
Evidence from recent water-borne disease outbreaks illustrates the importance of timeliness in health related warnings.
Timeliness of message delivery is dependent on how quickly a problem is identified, and how the message is delivered. The public can passively receive information on health related risks from the media or the utility, or actively seek out information from information sources such as the Internet, telephone hotlines or library services (Casman et al., 2000).
In determining when to go public with health advisories, health authoritiesreport that every outbreak of food- or water-borne illness must be examine dusing factors such as severity, potential impact and incubation time of the suspect pathogen. The health risk outcome of microbiological hazards to the public should be assessed, discussed and quantified among workers from diverse disciplines, including health officials, veterinarians, food processing experts, microbiologists, medical doctors, risk analysis experts, and consumer behavior experts.
Once sufficient evidence exists to issue a public health advisory, risk messages must be designed that accurately describe the risk to individuals and provide concrete steps that individuals can take to reduce the chances of risk exposure.
Further, the number of suspected or confirmed illnesses related to the particular outbreak should be included as a matter of course in any public communications. And once health advisories have been created, a variety ofmessage delivery techniques need to be employed, again depending on the severity of the hazard, the size of the impacted population and local circumstances.
For a severe and immediate hazard such as E. coli O157:H7 in drinking water, a mixture of low-to-high technology message delivery mechanisms should be employed, including door-to-door, the buddy system, the use of existing community networks such as Neighbourhood Watch, emergency hubsite information centers and even mobile megaphones, complimented by more broader mechanisms such as local media, posting information on a website, automated telephone messages, broadcast faxes, and electronic mail distribution.
However, the key to using any of these technologies effectively is to plan ahead and be prepared. Effective planning will establish which techniques are best for the size of the community and the existing infrastucture. No one technology can reach all members of the target audience, therefore combining delivery methods is essential.
The current state of risk management and communication research suggests that those responsible with food and water safety risk management must be actively seen to be reducing, mitigating or minimizing a particular risk. The components for managing the stigma associated with any food safety issue seem to involve all of the following factors:
effective and rapid surveillance systems;
effective communication about the nature of risk;
a credible, open and responsive regulatory system;
demonstrable efforts to reduce levels of uncertainty and risk; and,
evidence that actions match words.
This report has been concerned with the second point, the ability to effectively communicate about the nature of risk. E. coli O157:H7 is not regular E. coli. It is a highly virulent and dangerous pathogen that sickens tens of thousands annually in North America and kills hundreds. Each year since the 1993 Jack-in-the-Box outbreak has brought a high profile and deadly outbreak of E. coli O157:H7 from some corner of the developed world; outbreaks that receive significant media coverage and provide new insights; Australia in 1994 (involving the related E. coli O111); Scotland and Japan in 1996; a waterpark in Atlanta, Ga in 1998. While many Canadians may be unfamiliar with such outbreaks — media coverage in Canada is superficial at best, frequently focused on the hypothetical risks posed by various food-related technologies while ignoring the carnage associated with food and water-borne pathogens
Any local efforts must be supported by a national culture of awarenessregarding a risk such as E. coli O157:H7, which has been known to cause outbreaks and severe illness, and sometimes death, for almost 20 years. When compared to outbreaks and response in the U.S., it is observed that outbreaks, particularly of E. coli O157:H7 bring a sustained policy response from the highest levels of government, including the Office of the President. While there have been many private-sector initiatives in Canada to enhance the safety of the food supply, these efforts are rarely communicated or discussed by government, short of admonitions to “cook hamburger thoroughly.
As southeast Queensland experiences one of the wettest springs in years, rural residents are raising concerns about potentially contaminated drinking water after finding poisoned mice in their tanks, as the mouse plague continues to worsen.
Lucy Thackray of ABC reports frustrated landholders are continuing to try to reduce mice populations with rigorous baiting programs, but the problem isn’t showing any signs of slowing.
Louise Hennessy, from Elong Elong in Central West NSW, has issued a warning to other rural residents about potential health implications for humans and animals after finding baited mice in her drinking supply.
She made the discovery when she climbed up her house tank to check a blockage and was immediately overwhelmed by a revolting smell.
“It was so horrifying, I thought it would make a good picture to remind people to be vigilant about their water tanks,” Ms Hennessy said.
“We always filter the water going into our house from the tanks, so for us personally we feel we’ve covered our precautions so we didn’t notice anything with the taste. But the smell of the mice at the top of the tank was so disgusting.”
Dubbo Regional Council’s environment and health officer Simone Tenne said people often did not consider drinking water contamination.
“Rainwater tanks are perceived to be a clean source of drinking water, but they often have frogs in them, insects, a large amount of bird faeces which has come down off the roof,” Ms Tenne said.
“The public health sector recommends people do some form of treatment whether it be chlorination, a bit of acidification or some sort of filtration to avoid getting bacteria inadvertently through drinking contaminated water.”
Ms Tenne said health issues could be triggered by mice in drinking water.
Great source of Giardi. The Centers for Disease Control writes:
What is already known about this topic?
Giardiasis is a diarrheal disease caused by the parasite Giardia duodenalis, the most common cause of intestinal parasite infections in the United States.
Reported giardiasis outbreaks (N = 111), by mode of transmission* and year of earliest illness onset date — United States, 2012–2017
What is added by this report?
During 2012–2017, public health officials from 26 states reported 111 giardiasis outbreaks involving 760 cases. Leading causes of outbreaks were waterborne and person-to-person exposures. Private residences and child care facilities were the most common settings of giardiasis outbreaks across all transmission modes.
What are the implications for public health practice?
To prevent and control giardiasis outbreaks, CDC recommends prompt diagnosis, maintaining good hand hygiene, cleaning and disinfecting home environments and child care facilities, and monitoring water quality in private wells.
Giardiasis Outbreaks—United States, 2012-2017
Morbidity and Mortality Weekly Report
Erin E. Conners, PhD1,2; Allison D. Miller, MPH1; Neha Balachandran, MPH3; Brittany M. Robinson, MPH1; Katharine M. Benedict, DVM, PhD1
The Public Health Agency of Canada’s (PHAC) FoodNet Canada surveillance system (no, not that one, right, that’s the Canadian television network that wanted to sue me over video associated with 2004’s cooking show paper) is pleased to present this tables and figures report which provides the annual results of our surveillance activities conducted in 2019. The report is based on findings from its sentinel sites in British Columbia, Alberta, and Ontario. It also provides preliminary findings from Quebec, representing a partial year due to their implementation part way through the year in July 2019. The report focuses on trends in enteric pathogen disease rates, as well as trends in the prevalence of these pathogens found on potential disease sources: retail meats, manure from food producing animals and water. It is our hope that this report will be used to inform and shape discussions on food safety issues regarding enteric diseases and their sources.
Key findings:
In 2019, Campylobacter and Salmonella remained the most common causes of human enteric illness in the FoodNet Canada sentinel sites.
Travel continues to be an important factor in the burden of enteric disease. In 2019, approximately 30% of all cases of enteric disease were associated with travel outside of Canada.
Exposure to retail meat products remains a potential source of infection for human enteric illness. However, decreases in the prevalence of certain pathogen-food combinations were observed in 2019. For example, Salmonella on frozen breaded chicken products significantly decreased in 2019 compared to 2018 and is likely associated with interventions implemented at the industry level in 2019.
Other exposures, such as the farm environment and water, are also possible sources of infection for human enteric illness, with differences noted between the sites. For example, Salmonella is commonly found in broiler chicken manure, however, the prevalence significantly increased in BC whereas it significantly decreased in the AB site in 2019, resulting in an overall significant decrease in the combined sites.
The majority of clinical cases of shigatoxigenic Escherichia coli (STEC) were domestically acquired in 2019, with a significant increase in both travel and endemic incidence rates, which is primarily driven by the AB sentinel site who test all STEC-confirmed stool samples for non-O157 serogroups.
In 2019, surface water sampling was initiated for the first time in the ON site for STEC testing. The prevalence of STEC in the ON site (27%) was similar to the combined BC and AB irrigation water prevalence in 2019 (28%). · Continued monitoring of human illness and the potential exposures is important to ensure the continued health and safety of Canadians. The collection and integration of information across all of FoodNet Canada surveillance components (human, retail, on-farm, and water) in an enhanced and standardized way allows for the analysis of subtype distributions among human cases and potential exposure sources over time. This report will be followed by a comprehensive annual report, which will include more extensive analyses of temporal trends and subtyping information for an integrated perspective on enteric disease from exposure to illness.
Provision of safe drinking water in the United States is a great public health achievement. However, new waterborne disease challenges have emerged (e.g., aging infrastructure, chlorine-tolerant and biofilm-related pathogens, increased recreational water use).
Comprehensive estimates of the health burden for all water exposure routes (ingestion, contact, inhalation) and sources (drinking, recreational, environmental) are needed. We estimated total illnesses, emergency department (ED) visits, hospitalizations, deaths, and direct healthcare costs for 17 waterborne infectious diseases. About 7.15 million waterborne illnesses occur annually (95% credible interval [CrI] 3.88 million–12.0 million), results in 601,000 ED visits (95% CrI 364,000–866,000), 118,000 hospitalizations (95% CrI 86,800–150,000), and 6,630 deaths (95% CrI 4,520–8,870) and incurring US $3.33 billion (95% CrI 1.37 billion–8.77 billion) in direct healthcare costs.
Otitis externa and norovirus infection were the most common illnesses. Most hospitalizations and deaths were caused by biofilm-associated pathogens (nontuberculous mycobacteria, Pseudomonas, Legionella), costing US $2.39 billion annually.
Estimate of burden ad direct healthcare cost of infectious waterborne disease in the United States
Emerging Infectious Diseases vol. 2 no. 1
Sarah A. Collier , Li Deng, Elizabeth A. Adam, Katharine M. Benedict, Elizabeth M. Beshearse, Anna J. Blackstock, Beau B. Bruce, Gordana Derado, Chris Edens, Kathleen E. Fullerton, Julia W. Gargano, Aimee L. Geissler, Aron J. Hall, Arie H. Havelaar, Vincent R. Hill, Robert M. Hoekstra, Sujan C. Reddy, Elaine Scallan, Erin K. Stokes, Jonathan S. Yoder, and Michael J. Beach
Cryptosporidiosis is one of the leading causes of diarrhoeal illness and mortality induced by protozoan pathogens worldwide. As a largely waterborne disease, emphasis has been given to the study of Cryptosporidium spp. in surface waters, readily susceptible to pathogenic contamination. Conversely, the status of Cryptosporidium in potable groundwater sources, generally regarded as a pristine and “safe” drinking-water supply owing to (sub)-soil protection, remains largely unknown. As such, this investigation presents the first literature review aimed to ascertain the global prevalence of Cryptosporidium in groundwater supply sources intended for human consumption.
Thirty-seven peer-reviewed studies were identified and included in the review. Groundwater sample and supply detection rates (estimated 10–20%) indicate Cryptosporidium is frequently present in domestic groundwater sources, representing a latent health concern for groundwater consumers. Specifically, sample (10.4%) and source (19.1%) detection rates deriving from comprehensive “temporal” investigations are put forward as representative of a contamination ‘baseline’ for Cryptosporidium in ‘domestic’ groundwater supplies. Proposed ‘baseline’ prevalence figures are largely applicable in preventive risk-based catchment and groundwater quality management including the formulation of Quantitative Microbial Risk Assessment (QMRA). Notwithstanding, a large geographical disparity in available investigations and lack of standardized reporting restrict the transferability of research findings.
Overall, the mechanisms responsible for Cryptosporidium transport and ingress into groundwater supplies remain ambiguous, representing a critical knowledge gap, and denoting a distinctive lack of integration between groundwater and public-health sub-disciplines among investigations. Key recommendations and guidelines are provided for prospective studies directed at more integrative and multi-disciplinary research.
Cryptosporidium spp. in groundwater supplies intended for human consumption—a descriptive review of global prevalence, risk factors and knowledge gaps, 18 March 2020
Water Research
Chique; P. Hynds; L. Andrade; L. Burke; D. Morris; M.P. Ryan; J. O’Dwyer
Chapman used to write wonderful 1-page fact sheets that were used around the world, and maybe he can be persuaded to do so again, or find a skilled student.
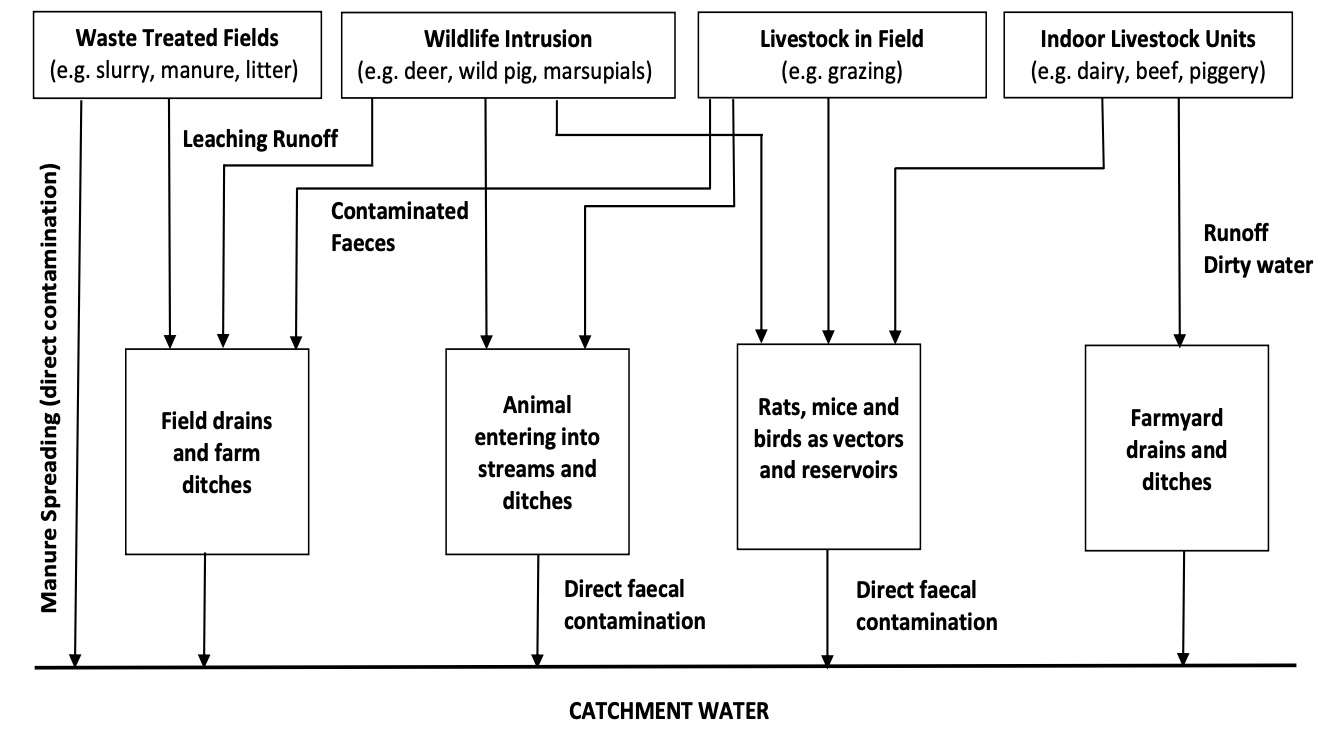
The important graphic is below. The rest is filler.
My friend Tim Caulfield, a Canada Research Chair in Health Law and Policy at the University of Alberta, author of “Is Gwyneth Paltrow Wrong About Everything?: How the Famous Sell Us Elixirs of Health, Beauty & Happiness” (Beacon, 2015) and host of “A User’s Guide to Cheating Death” on Netflix (that’s a long bio) writes for NBC News, humans need water but the marketing of water as a detoxifying, energizing, health-enhancing, miracle beverage has become a lucrative business. Over the past few years the booming wellness industry (aka Big Wellness) has coopted this most basic of biological needs to sell products and promises of miraculous improved health. But is there any evidence to support the hydration hype?
Before I dump on the water business, let’s give a nod to the positives. There is growing recognition that sugary beverages are not a good choice, nutrition wise. Evidence suggests that consumption of sugary beverages, especially soft drinks, is associated with a range of health issues, including obesity and heart disease. As a result, there is a broad consensus among nutrition and public health experts about the value of limiting the consumption of these calorie-dense and relatively nutrition-free beverages.
So, in this context, the shift to water is a very good thing. But that doesn’t mean we have to buy what the “premium” water market is selling.
But before we get to the fancy packaging, we need to talk about volume. Do you actually need to drink eight glasses of water a day? In a word: Nope.
This strange and incredibly durable myth seems to have emerged from a misinterpretation of a 1945 US Food and Nutrition Board recommendation. That document suggested a “suitable allowance of water for adults is 2.5 litres daily” (i.e., roughly eight glasses a day). But what is almost always overlooked is that the recommendation — which was not based on a robust body of research — also noted “[m]ost of this quantity is in prepared foods.” In other words, you already get the bulk of your needed water from the food you eat.
In reality, there is no magical amount of water. We do need to stay appropriately hydrated, of course. And as our climate and activities change, so does the amount of water we lose through sweating etc. But our bodies are good at telling us how much and when we should drink. (Thanks, evolution.) And all liquids — coffee, tea, that weird fluid inside hotdogs — count toward your daily consumption of water. My body can’t tell if an H20 molecule came from a fresh-water spring on the side of a remote Himalayan mountain or from a cup of gas station java (which isn’t, despite conventional wisdom to the contrary, dehydrating).
But even if water is found in a lot of foods and beverages, pure bottled water is still better for us, right? Wrong again.
Yes, drinking plain water is almost always a better choice than some other, sugar-infused, beverage. But the water you drink doesn’t need to come out of a plastic, glass, or 24-karat gold (yes, that is a thing) bottle.
Studies have shown that some people believe bottled water is healthier than tap water. That perception is wrong. In fact, tap water in the U.S. and Canada is almost always the best, cheapest and most environmentally friendly choice. Bottled water can be essential during emergencies that disrupt the supply of clean water. And there have been scary examples of contaminated public water — the Flint, Michigan water crisis being only one recent example.
We also need to be vigilant to ensure our public water supply remains clean. But in most places in the United States and Canada, tap water is tightly regulated and safe. Not only that, but tap water can have less contaminants than bottled water. A study from Canada, for example, found that 70 percent of the tested bottled water brands contained high levels of bacteria and generally had more bacteria than tap water. A 2019 Consumer Report investigation concluded “that in some cases bottled water on store shelves contains more potentially harmful arsenic than tap water.”
But bottled water tastes better, you say! Actually, blind taste tests have consistently found that to be untrue too. To cite just one example, only one-third of the participants in a Boston University study, were able to correctly identify tap water. One third thought it was bottled water and one third couldn’t tell the difference.
But bottled water tastes better, you say! Actually, blind taste tests have consistently found that to be untrue too.
And now we get to what is probably the biggest scam. Wellness wonks have been pushing absurd diets, supplements and potions for decades. Now that same thinking has come to water, with alkaline, hydrogen, gluten and GMO-free water brands hitting the supermarket and health food store shelves near you.
Nope, nope and — sigh — nope.
Alkaline water is part of the larger multimillion-dollar alkaline diet fad embraced by celebrities like New England Patriots quarterback Tom Brady. Proponents claim that humans can become too acidic and, as such, we need to consume foods and beverages that will lower the pH of our bodies. By doing so, we will improve our health and reduce the incidence of disease and cancer, the theory goes.
Problem one: There is little evidence to support the entire premise that adjusting the pH of your food will have an impact on our health. And the studies that have explored the claim have found little benefit to this dietary approach, outside of the diet’s push to eat more fruits and vegetables. (Eating more fruits and vegetables is of course good for you hand can help you stay healthier for longer.)
Problem two: You can’t change the pH of your body through food and beverages. So the entire premise is scientifically absurd. Your body tightly regulated the pH of your blood. It doesn’t need the help of overpriced bottled water.
In the spring of 2018, an E. coli O157 outbreak linked to romaine lettuce grown in the Yuma, Arizona area resulted in 210 reported illnesses from 36 states, 96 hospitalizations, 27 cases of hemolytic uremic syndrome (HUS) and five deaths.
The U.S. Food and Drug Administration has launched a new initiative with support from the Arizona Department of Agriculture, and in conjunction with the University of Arizona Cooperative Extension, the Wellton-Mohawk Irrigation and Drainage District (WMIDD), and members of the Yuma area leafy greens industry to better understand the ecology of human pathogens in the environment in the Yuma agricultural region. This initiative will be a multi-year study which will focus on how these pathogens survive, move and possibly contaminate produce prior to harvest.
While the FDA, the Arizona Department of Agriculture and other state partners conducted an environmental assessment from June through August 2018 that narrowed the scope of the outbreak, the specific origin, the environmental distribution and the potential reservoirs of the outbreak strain remain unknown.
Between 2009 and 2017, FDA and partners at CDC identified 28 foodborne STEC outbreaks with known or suspected links to leafy greens. Like a lot of fresh produce, leafy greens are often eaten raw without a kill-step, such as cooking, that could eliminate pathogens that may be present.
Sounds like Yuma growers could use a Box of Rain. Or maybe more knowledge of the microbial ripple effect. May death be groovy for you, long-time Grateful Dead collaborator and lyricist Robert Hunter, who passed on Tuesday, aged 78.
The U.S. Centers for Disease Control reports that waterborne hepatitis A outbreaks have been reported to CDC. Person-to-person transmission of hepatitis A has increased in recent years.
Reported drinking water–associated hepatitis A outbreaks have declined since introduction of universal childhood vaccination recommendations and public drinking water regulations. However, unvaccinated persons who use water from untreated private wells remain at risk.
Public health officials should raise awareness of risks associated with untreated ground water among users of private wells and of options for private well testing and treatment. Water testing and treatment are important considerations to protect persons who use these unregulated systems from HAV infection.
Hepatitis A virus (HAV) is an RNA virus primarily transmitted via the fecal-oral route and, in rare cases, causes liver failure and death in infected persons. Although drinking water–associated hepatitis A outbreaks in the United States are rarely reported (1), HAV was the most commonly reported etiology for outbreaks associated with untreated ground water during 1971–2008 (2), and HAV can remain infectious in water for months (3). This report analyzes drinking water–associated hepatitis A outbreaks reported to the Waterborne Disease and Outbreak Surveillance System (WBDOSS) during 1971–2017. During that period, 32 outbreaks resulting in 857 cases were reported, all before 2010. Untreated ground water was associated with 23 (72%) outbreaks, resulting in 585 (68.3%) reported cases. Reported outbreaks significantly decreased after introduction of Advisory Committee on Immunization Practices (ACIP) hepatitis A vaccination recommendations* and U.S. Environmental Protection Agency’s (USEPA) public ground water system regulations.† Individual water systems, which are not required to meet national drinking water standards,§ were the only contaminated drinking water systems to cause the last four reported hepatitis A outbreaks during 1995–2009. No waterborne outbreaks were reported during 2009–2017. Water testing and treatment are important considerations to protect persons who use these unregulated systems from HAV infection.
U.S. states and territories have voluntarily reported waterborne disease outbreaks to WBDOSS since 1971.¶ Waterborne hepatitis A outbreaks (1971–2017) reported as of March 13, 2018, were reviewed. An outbreak of hepatitis A was defined as two or more cases of HAV infection epidemiologically linked by time and location of water exposure. To compare occurrence with other waterborne exposure pathways, outbreaks reviewed included those caused by drinking, recreational, environmental (i.e., nondrinking, nonrecreational water), or undetermined water exposures.** As described previously (1), data reviewed included location; date of first illness; estimated number of primary cases, hospitalizations, and deaths; water system type according to USEPA Safe Drinking Water Act definitions (i.e., community, noncommunity, and individual); setting of exposure; drinking water sources (i.e., ground water, surface water, and unknown); and water system characteristics.†† Community and noncommunity water systems are public water systems that have 15 or more service connections or serve an average of 25 or more residents for ≥60 days per year.§§ A community water system serves year-round residents of a community, subdivision, or mobile home park. A noncommunity water system serves an institution, industry, camp, park, hotel, or business. Individual water systems are small systems (e.g., private wells and springs) not owned or operated by a water utility that have fewer than 15 connections or serve fewer than 25 persons. The number of outbreaks before and after public health interventions were compared; chi-squared tests were used to identify significant (p-value<0.05) differences. Data were analyzed using SAS software (version 9.4; SAS Institute) and visualized in ArcGIS (version 10.6.1; Environmental Systems Research Institute).
Thirty-two drinking water–associated hepatitis A outbreaks were reported to CDC during 1971–2017; the last one occurred in 2009 (Table). These drinking water–associated outbreaks accounted for 857 cases (range = 2–50), with no reported deaths. Data on number of deaths were unavailable for three outbreaks. Data on hospitalizations were unavailable for all outbreaks. Outbreaks occurred in 18 states, all in the lower continental United States (Figure 1). One environmental outbreak (1975) and one recreational water outbreak (1989) were reported during this period, but were excluded from this analysis.
The most commonly reported water system type associated with an outbreak was individual, accounting for 13 of 32 (41%) outbreaks and 257 of 857 (30.0%) cases, followed by community (10 [31%] outbreaks; 241 [28.1%] cases) and noncommunity (9 [28%] outbreaks; 359 [41.9%] cases). All individual water systems with outbreaks were supplied by private wells or springs. The majority of all drinking water outbreaks and cases were associated with systems supplied by ground water (30 [94%] outbreaks; 804 [93.8%] cases) and with an absence of water treatment (23 [72%] outbreaks; 585 [68.3%] cases).
The incidence of reported drinking water–associated hepatitis A outbreaks significantly decreased after introduction of the 1989 USEPA Total Coliform and Surface Water Treatment Rules (77% decline from 1971–1989 [24 outbreaks] to 1990–2017 [eight]; p = 0.003), the 1996 ACIP hepatitis A vaccination recommendations (87% decline from 1971–1996 [29] to 1997–2017 [three]; p<0.001), and the 2006 Ground Water Rule and expanded ACIP vaccine recommendations (78% decline from 1971–2006 [30] to 2007–2017 [two]; p = 0.038) (Figure 2). From 1995 through 2009, all four hepatitis A drinking water–associated outbreaks, resulting in 35 cases, were attributed to individual water systems using untreated ground water sources. No water-associated hepatitis A outbreaks have been reported since July 2009.
Reported drinking water–associated hepatitis A outbreaks have declined since reporting began in 1971, and none have been reported since 2009, mirroring the overall decline in U.S. cases (4,5). Vaccination for hepatitis A, combined with USEPA regulations that require testing and, where necessary, corrective actions or treatment for drinking water supplies, likely played a role in reducing reported hepatitis A drinking water–associated outbreaks.
Vaccination efforts have led to significant changes in hepatitis A epidemiology (4,6,7). HAV infection rates in the United States have decreased since the introduction of hepatitis A vaccine in 1995 (4,5). Vaccine recommendations were originally targeted to children in communities with high rates of hepatitis A infections west of the Mississippi and other groups at risk (e.g., international travelers, men who have sex with men, illicit drug users, persons with clotting factor disorders, and persons with occupational risk). By 2006, routine hepatitis A vaccination was recommended for all children aged ≥l year regardless of geographic area of residence (5). Although vaccination was never recommended for users of individual ground water systems, this group likely benefited from the recommendations targeting children and other groups at risk. Incidence of HAV infection is now lowest among persons aged 0–19 years (4). However, the proportion of HAV-associated hospitalizations steadily increased during 1999–2011, likely because of more severe disease in older adults, with persons aged ≥80 years experiencing the highest rates of infection (6). The number of hepatitis A cases in the United States reported to CDC increased by 294% during 2016–2018, compared with the period 2013–2015 (8), primarily because of community-wide outbreaks in persons reporting homelessness or drug use (7). ACIP recommends vaccination to persons who use drugs and recently expanded recommendations to persons experiencing homelessness.¶¶
Reported drinking water–associated hepatitis A outbreaks were most commonly linked to individual water systems that used wells with untreated ground water. Recreational and environmental outbreaks were only reported twice, suggesting that drinking water is a more common waterborne exposure pathway for hepatitis A. Nearly 43 million U.S. residents, or 13% of the population, are served by individual water systems, primarily from ground water sources (https://pubs.er.usgs.gov/publication/cir1441external icon). Untreated ground water sources were associated with 30% of all drinking water–associated outbreaks reported to CDC during 1971–2008 (1). The USEPA Total Coliform and Surface Water Treatment Rules of 1989 and Ground Water Rule of 2006 provide enhanced safety measures for public water systems using ground water sources and might have contributed to the absence of reported hepatitis A outbreaks linked to community water sources since 1990. However, federal regulations do not apply to individual water systems, which often have inadequate or no water treatment (9). Private wells or springs were the only contaminated drinking water systems to cause the last four reported hepatitis A outbreaks during 1995–2009. CDC recommends that owners of private wells test their water annually for indicators of fecal contamination (https://www.cdc.gov/healthywater/drinking/private/wells/testing.html). Factors contributing to fecal contamination of ground water include nearby septic systems or sewage, weather patterns (e.g., heavy rainfall), improper well construction and maintenance, surface water seepage, and hydrogeologic formations (e.g., karst limestone) that allow for rapid pathogen transport (2,9).
The findings in this report are subject to at least three limitations. First, waterborne hepatitis A outbreak reporting is through a passive, voluntary surveillance system; health departments have varying capacity to detect, investigate, and report outbreaks, which might result in incomplete data on outbreak occurrence and characteristics within and across jurisdictions. Thus, outbreak surveillance data might underestimate the actual number of drinking water–associated hepatitis A outbreaks and might underreport information regarding health outcomes such as cases of illness. Second, attributing the source of an outbreak to individual water systems can be particularly difficult because hepatitis A can also be spread through person-to-person transmission within a household. Finally, outbreak data before 2009 did not include case-specific information; thus, demographic factors, including age, could not be assessed.
Drinking water–associated hepatitis A outbreaks have declined and essentially stopped, likely in large part because of the introduction of an efficacious vaccine as part of the routine childhood immunization program and microbial drinking water regulations for public water systems. The degree to which these interventions have contributed to the decline in outbreaks is uncertain. However, waterborne outbreak surveillance data is not yet finalized for 2018, and the recent increase in person-to-person transmission of hepatitis A (7,8) has the potential to cause a resurgence in waterborne outbreaks through increased fecal HAV contamination of private ground water supplies. Outbreak data suggest that individual water systems, primarily those systems drawing untreated ground water from wells, pose the highest risk for causing drinking water–associated hepatitis A outbreaks. These systems are not regulated by USEPA; CDC recommends that owners evaluate their well water quality at least yearly. If indicators of fecal contamination are detected, remediation and treatment of private well water is recommended. Guidance on private well testing and treatment solutions for microbial contamination is provided by USEPA (https://www.epa.gov/privatewells/protect-your-homes-waterexternal icon) and CDC (https://www.cdc.gov/healthywater/drinking/private/wells/index.html). Although the current nationwide outbreak of hepatitis A is not water-associated, considering ground water as a possible transmission route is warranted during community-wide outbreaks of hepatitis A. Ground water can be contaminated with HAV during community transmission of hepatitis A, increasing the risk for persons using untreated water. Public health education about the risks associated with drinking untreated ground water from individual systems, as well as relevant safety measures (i.e., water testing, water treatment, and vaccination), is needed to prevent future drinking water–associated hepatitis A outbreaks.
US: Impact of public health interventions on drinking water-associated outbreaks of hepatitis A-United States, 1971-2017