Only Washington-types could take a story about recent successes and failures in foodborne illness rates and surveillance – 18 fascinating papers — and turn it into a whine about how lobbyists were excluded from access, ahead of mere mortals.
The Washington Post reports that unlike last year, the U.S. Centers for Disease Control released the data without reaching out to consumer groups and other key stakeholders who typically are .jpg) notified in advance. Instead, the charts and graphs were quietly posted online Friday.
notified in advance. Instead, the charts and graphs were quietly posted online Friday.
I’m not sure who these key stakeholders are, and how many of them are self-proclaimed. The solution is for CDC to publish a press release summarizing the findings, note their existence, and releasing it to everyone at the same time.
And only in Washington would people whine that delayed passage of the Food Safety Modernization Act is leading to increases in foodborne illness.
“Everyone was hoping that this new food safety law would be in place and we’d start seeing improvements by now,” said Erik Olson, a director at the Pew Health Group. “What these CDC numbers show is that unless new protections are put into place, millions of Americans are going to continue to get sick from contaminated food.”
I’m immediately suspicious of people who speak on behalf of everyone (and people who say trust me). I have yet to see a credible, detailed analysis that shows FSMA will lower rates of foodborne illness.
But that’s the bizness of Washington. They don’t seem good at it.
Four years ago, the CDC numbers yielded the same story – rates were stagnant, but still way too many sick people. There is no evidence educational campaigns do anything except make people feel like they are doing something, there is no evidence legislation does much, yet that’s always the punchline: we need more laws, we need more education.
Doesn’t work.
We need new messages using new media to really create a culture that values microbiologically safe food.
That’s what I said four years ago, it could have been 20 years ago. Same as it ever was.
The most recent figures from the Centers for Disease Control and Prevention show that the rates of infections linked to four out of five key pathogens it tracks — salmonella, vibrio, .jpg) campylobacter and listeria — remained relatively steady or increased from 2007 through 2011. The exception is a strain of E. coli, which has been tied to fewer illnesses in the same time frame.
campylobacter and listeria — remained relatively steady or increased from 2007 through 2011. The exception is a strain of E. coli, which has been tied to fewer illnesses in the same time frame.
The CDC found that the most frequent cause of infection in 2011 was salmonella, followed by campylobacter.
Below are actual excerpts from the CDC summary report. All 18 abstracts will appear on bites-l as soon as I complete a long plane ride, custom(s) probing, and return to the land of unlimited Internet.
Foodborne disease is an important public health problem in the United States, with an estimated 9.4 million domestically acquired illnesses and 1351 deaths from known pathogens each year. The Foodborne Diseases Active Surveillance Network (FoodNet) tracks important foodborne illnesses, generating information that provides a foundation for food safety policy and prevention efforts. FoodNet has provided information that contributes to food safety efforts by estimating numbers of foodborne illnesses, monitoring trends in incidence of specific foodborne illnesses over time, attributing illnesses to specific foods and settings, and disseminating information. Since it started in 1996, FoodNet has been an excellent example of partnership among federal and state agencies. This Clinical Infectious Diseases supplement contains a variety of articles that provide new information on current issues; together, they highlight FoodNet’s central role in U.S. surveillance and investigation of foodborne disease.
FoodNet’s core work is ongoing active, population-based surveillance for laboratory-confirmed infections caused by 9 pathogens transmitted commonly through food, as well as for hemolytic uremic syndrome. Several articles in this supplement report on these core data, examining trends and providing regulatory and public health agencies, industry, and consumer groups with data needed to prioritize and evaluate food safety interventions and monitor progress toward national health objectives. For example, Ong et al report the dramatic decline in Yersinia enterocolitica infections since 1996, particularly among young black children. Not all the news is good, however; Newton et al [analyze data from FoodNet and the Cholera and Other Vibrio Illness Surveillance System (COVIS), showing that Vibrio infections have increased nationally. Two articles in this supplement examine FoodNet surveillance data on invasive listeriosis. The article by Silk et al summarizes trends in surveillance data from 2004 to 2009, whereas Pouillot et al use FoodNet surveillance data to estimate the relative risk of listeriosis by age, pregnancy, and ethnicity, providing new insights into variations in risk across the population. Together, these articles emphasize that to substantially decrease the incidence of listeriosis, prevention measures should target higher-risk groups, particularly pregnant women, especially Hispanics, and older adults. Hall et al examine trends in Cyclospora infection, showing that outbreaks and international travel play an unusually large role in the epidemiology of these infections and suggesting that prevention efforts would most effectively focus on foods from and travel to endemic areas.
FoodNet continuously works to improve the quality of its surveillance data and methods for analysis. In this supplement, Henao et al describe the methods and rationale surrounding the introduction, in 2011, of a measure of overall change in the incidence of infection over time using surveillance data on infections caused by 6 bacterial pathogens. This measure, which provides a comprehensive picture of changes in incidence of foodborne infections, documents a 23% decline overall in incidence for these pathogens in 2010 compared with the first 3 years of surveillance (1996–1998). Although it does not replace pathogen-specific trend data, this summary measure can help inform the development and assessment of policies and interventions  to prevent foodborne illness. Another article, by Manikonda et al, reports on a study to validate the reporting of deaths in FoodNet surveillance, an important issue because deaths, although rare, are disproportionately responsible for the economic and human costs of foodborne disease. Finally, Ong et al examine the impact of case ascertainment strategies and case definitions on surveillance for pediatric hemolytic uremic syndrome in FoodNet.
to prevent foodborne illness. Another article, by Manikonda et al, reports on a study to validate the reporting of deaths in FoodNet surveillance, an important issue because deaths, although rare, are disproportionately responsible for the economic and human costs of foodborne disease. Finally, Ong et al examine the impact of case ascertainment strategies and case definitions on surveillance for pediatric hemolytic uremic syndrome in FoodNet.
Several articles in the supplement elucidate aspects of the “surveillance steps” that are necessary for a case of infection to be ascertained by FoodNet surveillance. FoodNet and many other surveillance systems for bacterial enteric infections are based on culture-confirmed infections, so FoodNet surveillance data must be interpreted in the context of the “surveillance steps” that lead to culture confirmation: the ill person must seek medical care, a stool specimen must be submitted, and the clinical laboratory must test for and identify the pathogen. In particular, the recent and ongoing shift among clinical laboratories toward culture-independent methods for detecting enteric pathogens is of great importance.
In 2011, the CDC released new estimates of the number of foodborne illnesses in the United States, the Food Safety Modernization Act was signed into law, and new national health objectives for foodborne illness were set as part of the Healthy People 2020 goals. All of these initiatives, as well as continued concern about food safety on the part of the public and policy makers, emphasize the need for precise and accurate information about foodborne disease. Regulators and other public health officials, consumer advocates, industry, and others need information on trends, high-risk populations, and the foods causing illness so that interventions can be targeted most efficiently and effectively. FoodNet provides the articles in this supplement as part of its efforts to disseminate the results of its surveillance and analytic work. Although FoodNet surveillance is conducted in a geographic area that covers only 15% of the US population, the data it generates are a valuable resource for the entire United States. The FoodNet program shows the impact that high-quality, nationally coordinated surveillance can have on public health and policy.

 But that would require imagination, creativity and commitment, the things that get stifled in any kind of bureaucracy.
But that would require imagination, creativity and commitment, the things that get stifled in any kind of bureaucracy. Yersinia was unchanged. These findings highlight the need to continue to identify and address food safety gaps that can be targeted for action by the food industry and regulatory authorities.
Yersinia was unchanged. These findings highlight the need to continue to identify and address food safety gaps that can be targeted for action by the food industry and regulatory authorities.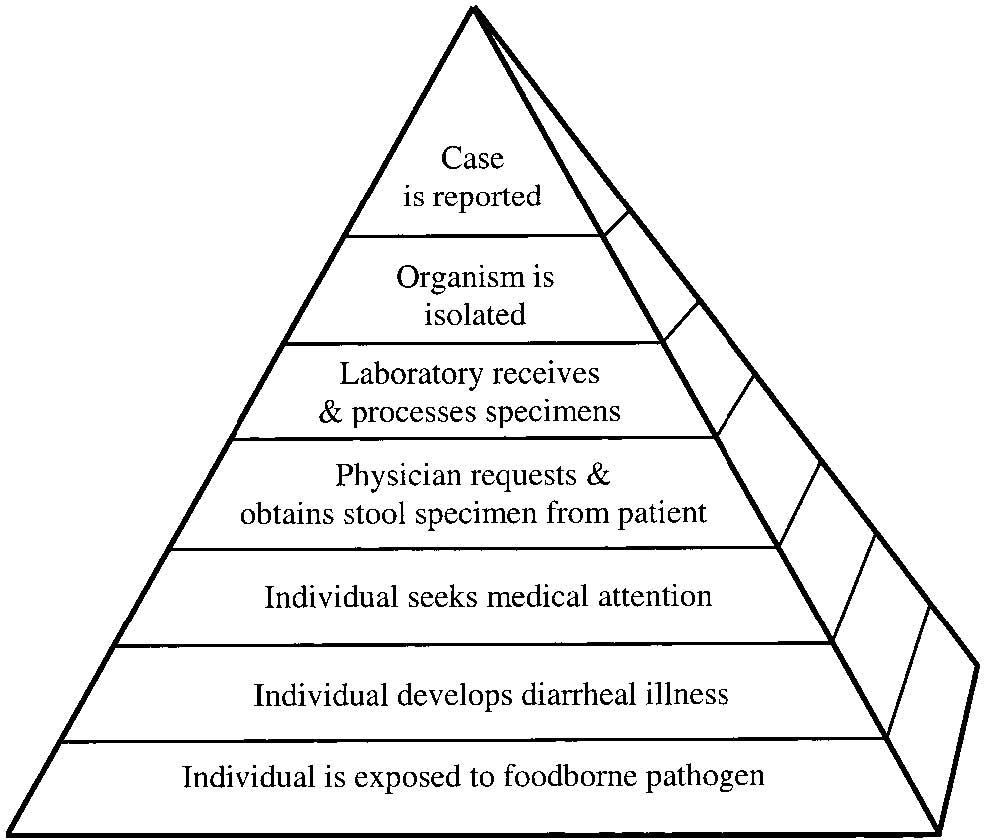


.jpg) My whiny kid didn’t help either.
My whiny kid didn’t help either..jpg) Modernization Act, which will raise the level of attention that food producers, processors, distributors and importers must give to ensuring their products are safe for human and animal consumption.
Modernization Act, which will raise the level of attention that food producers, processors, distributors and importers must give to ensuring their products are safe for human and animal consumption..jpg) mortality and hemolytic uremic syndrome (HUS) rates observed in healthy adults.
mortality and hemolytic uremic syndrome (HUS) rates observed in healthy adults..jpg) involved in adhesion or invasion.
involved in adhesion or invasion.  of animal origin: monitoring and evaluation contains 13 research papers.
of animal origin: monitoring and evaluation contains 13 research papers.
.jpg) analysis approach to problems: this is what we know, these are the assumptions we made, this is what we think it means, let’s discuss how to make it better.
analysis approach to problems: this is what we know, these are the assumptions we made, this is what we think it means, let’s discuss how to make it better.