CBS Local reports that with food delivery platforms like Uber Eats, GrubHub and Postmates bursting at the seams, we wanted to know what some delivery people were doing with your food before you took a bite.
One food delivery driver – whose identity is concealed – told CBSLA’s David Goldstein he’s heard drivers talk about helping themselves to your order.
“Taking sips of soda all the time….sticking a straw in it and drinking it and putting another top on it,” he said.
So Goldstein’s team set up hidden cameras in restaurants and watched as food delivery people came to pick up – many of whom walked out with open bags where they can easily taste your food.
Cameras caught one man pick up a delivery order at a Fatburger restaurant in North Hollywood. After he put the bag on the front seat of his car, he proceeded to eat what looks like French fries.
As he backs out, he appears to put another fry into his mouth.
He proceeded to make two deliveries within minutes. On the first, the driver was seen wiping his fingers on his leg and then appears to lick them clean in his mouth.
The second delivery was the Fatburger order to a house in North Hollywood.
Goldstein then showed the video to Naimie Ojeil, who said the order was for his teenage kids.
“Horrible, disgusting,” he said.
When Goldstein confronted the driver at a later date, he didn’t have much to say.
Cameras caught another driver pick up a delivery, placing the bag on the passenger seat in his car, and then a minute or so later, he moves the bag, puts his hand inside and grab some fries before he drives away.
Wheat flour has recently been recognised as an exposure vehicle for the foodborne pathogen Shiga toxin-producing Escherichia coli (STEC). Wheat flour milled on two sequential production days in October 2016, and implicated in a Canada wide outbreak of STEC O121:H19, was analysed for the presence of STEC in November 2018.
Stored in sealed containers at ambient temperature, the water activity of individual flour samples was below 0.5 at 6 months post-milling and remained static or decreased slightly in individual samples during 18 months of additional storage. STEC O121 was isolated, with the same genotype (stx2a, eae, hlyA) and core genome multilocus sequence type as previous flour and clinical isolates associated with the outbreak. The result of this analysis demonstrates the potential for STEC to persist in wheat flour at levels associated with outbreak infections for periods of up to two years. This has implications for the potential for STEC to survive in other foods with low water activity.
Shiga toxin-producing Escherichia coli survives storage in wheat flour for two years
This study was conducted to validate a simulated commercial baking process for plain muffins against E. coli O121 (isolated from the recent illness outbreak associated with flour), and compare the thermal inactivation parameters (D- and z-values) of cocktails of four isolates of E. coli O121 and three serovars of Salmonella (Newport, Typhimurium, and Senftenberg) in muffin batter.
Flour samples were spray inoculated with the E. coli O121 or Salmonella cocktails, dried back to the pre-inoculation weight to achieve ~7 log10 CFU/g, and used to prepare muffin batter. For the muffin baking validation study using E.coli O121, muffin batter was baked at 375 °F (190.6 °C) oven temperature for 21 min followed by 30 min of ambient cooling. The E. coli O121 population decreased by >7 log10 CFU/g in muffins by 17 min of baking, and was completely eradicated after 21 min of baking and ambient cooling. The D-values of E. coli O121 and Salmonella cocktails in muffin batter at 60, 65 and 70 °C were 42.0 and 38.4, 7.5 and 7.2, and 0.4 and 0.5 min, respectively; whereas the z-values of E. coli O121 and Salmonella were 5.0 and 5.2 °C, respectively.
Comparison of survival and heat resistance of Escherichia coli O121 and salmonella in muffins
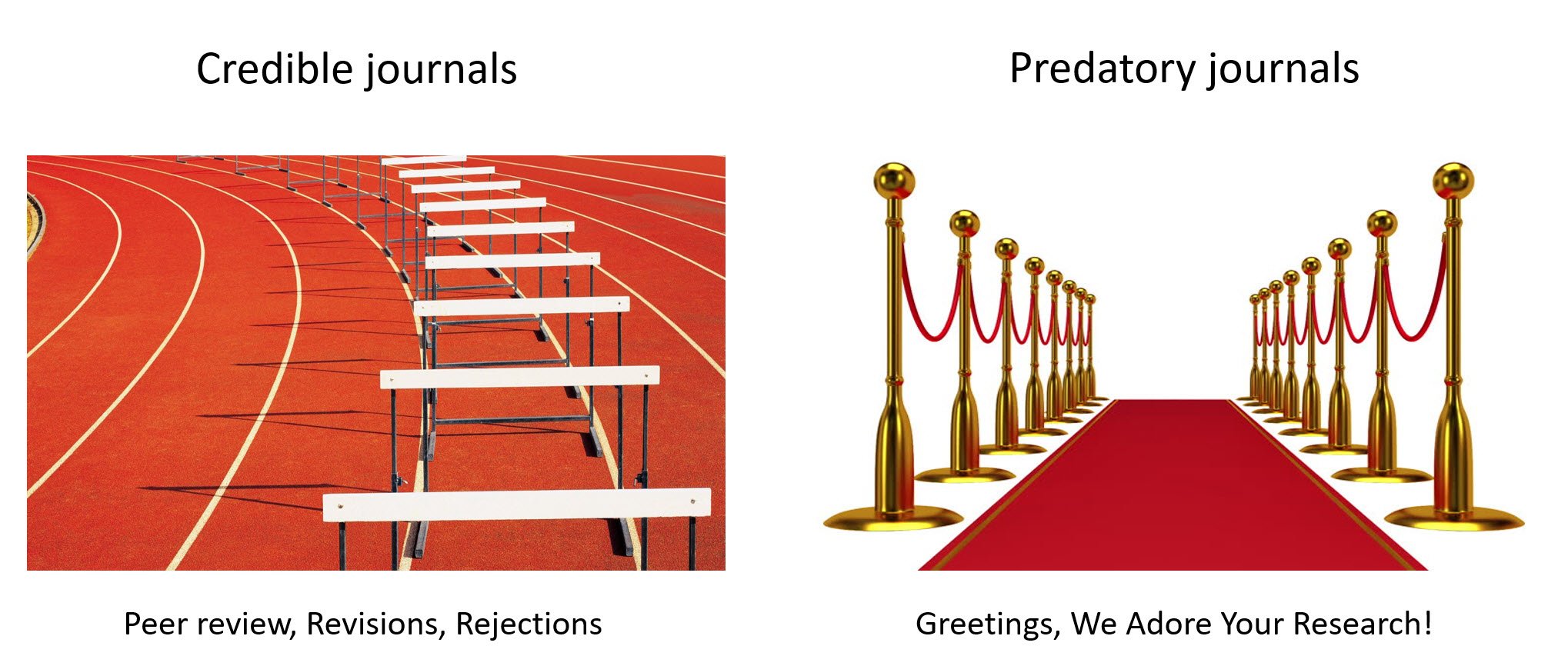
No good journal does that. They have lots of submissions.
The spam emails highlight the wild west of predatory journals, often with names that try to imitate real journals. Today’s was the “New American Journal of Medicine”, a not-so-subtle variation of the New England Journal of Medicine or the American Journal of Medicine. It looks like that journal has published a total of 8 papers in 2019. I looked at one of them and ‘crap’ is my generous assessment. It’s a paper that recommends a treatment for pregnant women and it’s one page long, does not disclose the funding source, fails to fulfill pretty much every standard reporting requirement for a clinical trial and reports essentially no specific data or analysis. But, it’s ‘published data’ and on someone’s CV.
The state of the scientific literature is pretty messed up. “Show me the study” has been a common refrain, but it’s not as useful these days because anything can get published.
Why?
Too many journals.
Predatory journals.
Profit.
Good journals screen out the weak articles. High impact journals publish a minority (5-25% of submissions…and most often people only send their best papers to those journals). Some journals are still good quality and take lower impact papers that are still good science. Some journals take whatever they can get, trying to screen out the bad science.
Others…they take whatever they can get, as long as the authors can pay. Sadly, there are literally thousands of those.
Some people don’t realize we don’t get paid to write scientific papers. Some journals publish at no cost, but increasingly, there are publication fees that may range from a few hundred to a few thousand dollars. That, itself, isn’t necessarily the problem. Some journals charge fees so that the papers can be open access (available to anyone, without a need for a subscription). However, some journal charge a couple thousand dollars, make a nice profit and don’t particularly care about the science.
As someone who’s an associate editor, editorial board member and frequent reviewer for many journals, I see the good and bad.
I see papers that should be published accepted.
I see good quality papers rejected by good journals, knowing they’ll still end up in another good journal.
I see bad papers rejected.
However, I also see…
Horrible quality papers rejected that I know will end up published somewhere.
It’s frustrating to be reviewing a paper that’s complete crap, knowing it will find a home in a journal eventually. Yes, it will most likely be in a bottom feeder journal that many of it of us in the scientific community know is dodgy. However, not everyone will realize that and there will still be ‘published data’ to refer back to. Sometimes, that’s just frustrating, because poor quality science shouldn’t be published. However, when it deals with clinical matters (e.g. diagnosis, treatment…) it can be harmful, since poor quality or invalid data shouldn’t form the basis of decisions. Yet, it happens.
There have been a couple ‘stings’, where fake (and clearly garbage) papers have been submitted to journals. The highest profile was one that was published in Science (Bohannon, 2013). The author submitted a paper to various journals, with the following set-up “Any reviewer with more than a high-school knowledge of chemistry and the ability to understand a basic data plot should have spotted the paper’s short-comings immediately. Its experiments are so hopelessly flawed that the results are meaningless.” More than 50% of open access journals accepted it.
There are many reasons these dodgy journals are used.
“Publish or perish” isn’t quite true but it’s pretty close. Junior faculty need to show productivity to keep their positions or move into the increasingly elusive tenured positions. Scientific papers is a key metric, because it’s easy to count.
Some people get taken advantage of, not realizing the journal is predatory (or that fees are so high, until after the paper is accepted).
Commercial profit. Companies want to say their products are supported by published data. If the data aren’t any good, the amount of money that it takes to get something published is inconsequential for most companies.
Open access isn’t inherently bad. There are excellent open access journals that charge a couple thousand dollars per paper but have high standards. Open access is ideal as it means the science is available to everyone. It just has to be acceptable science, and that’s where things start to fall apart.
Anyway…enough ranting. I always like to say “don’t talk about a problem without talking about a solution” but I don’t have an easy solution. More awareness is the key, which is why sites that track predatory journals, such as Beall’s List, are important. It’s a good update on a sad state of affairs.
This is not food safety but could be. A colleague never knew this story, so I found it and shared it with him.
And know all of youse who don’t like it, start your own blog.
Oh, and hit delete.
That’s me and grandma, 1963.
Wrote this for the Globe and Mail in 1994
How We Die
Reflections on Life’s Final Chapter
Sherwin B. Nuland
1994
Alfred A. Knopf
278 pages
A Gentle Death
Marilynne Seguin, R.N.
1994
Key Porter Books
249 pages
$19.95
Review by Douglas Powell
My grandmother ended her own life. After five years of painstaking care for her husband, who was slowly deteriorating from the cerebral ravages of Alzheimer’s disease, she decided that a sixth was not worth facing.
Her death was quick and without warning. One moment we were saying goodbye before a routine trip to the store, the next I was transferring her from car to wheelchair at the hospital emergency ward. Within 30 minutes she was officially deceased, the result of a major pharmaceutical overdose.
Looking back, I’ve often wondered what I would say to her, given the chance. Don’t do it, life is really okay. You are not alone. Things will get better.
But in reality, life is often harsh, she was often alone, and the prospects of yet another winter, trekking to the hospital each day to watch the person she had spent the vast majority of her life with become even more unfamiliar, meant that things certainly were not about to get better; at least not in any foreseeable future.
Western society is finally being forced to grapple with some of the difficult consequences that arise when medical technology conflicts with individual rights and freedoms. In Canada, Nancy B., a 25 year-old quadriplegic, and Sue Rodriquez, who suffered from the degenerative wasting of Lou Gehrig’s disease, have challenged existing laws and brought the question of when to say enough is enough to the arena of public debate. The discussion is welcome and the only antidote to the private anguish of such decisions, as is forcefully brought home in two new books.
Humans have created powerful myths and rituals to accompany death, writes Sherwin Nuland in How We Die, but perhaps none more bizarre than the modern hospital, “where it can be hidden, cleansed of its organic blight, and finally packaged for modern burial. We can now deny the power not only of death but of nature itself. We hide our faces from its face, but still we spread our fingers just a bit, because there is something in us that cannot resist a peek.”
Dr. Nuland, a physician who has authored several books about the medical profession and continues to teach surgery and the history of medicine at Yale University, says this book was written to demythologize the process of dying, to present it in its biological and clinical realities. The changes at a cellular and organ-level that accompany heart attacks, stroke and cancer are presented in detail that may be intimidating to the uninitiated. Then again, any person who is faced with life-threatening disease can quite rapidly assimilate the medical jargon — they have to. Physicians capable of talking in clear, simple language are rare.
Nuland is blunt. Despite the gripping television constructs, few of the 350,000 Americans who suffer cardiac arrest each year actually survive. Nuland observes that after the vain attempts at resuscitation, the critical response team eventually stops and the mood is transformed from heroic rescue to dejected gloom of failure. But it’s the patient and their families that Nuland, like any good — and increasingly rare — general practitioner focuses on. “The patient dies alone among strangers: well-meaning, empathetic, determinedly committed to sustaining his life — but strangers nonetheless. There is no dignity here.”
Then there’s the story of Dr. Nuland as young intern and his first crisis when a patient went into massive cardiac. Using all his training, Nuland opened the man’s chest and began to massage his heart, as was the routine practice at the time, but to no avail. The man died. Yet suddenly he “threw back his head once more and, staring upward at the ceiling with the glassy unseeing gaze of open dead eyes, roared out to the distant heavens a dreadful rasping whoop that sounded like the hounds of hell were barking. Only later did I realize that what I heard was McCarty’s version of the death rattle, a sound made by spasm in the muscles of the voice box, caused by the increased acidity in the blood of a newly dead man. It was his way, it seemed, of telling me to desist — my efforts to bring him back to life could only be in vain.” Or, as Nuland constantly reminds the reader, “we rarely go gentle into that good night.”
Marilynne Seguin’s A Gentle Death is an attempt to help ease that journey for patients and their families. Sequin, a registered nurse for over 30 years as well as a founding member and executive director of the Toronto-based Dying With Dignity tells how she, like Nuland, was trained to prolong life at all costs. Experience has taught her to question prevailing attitudes of the medical establishment and she stresses that patients must become informed and responsible for the medical decisions that affects their lives.
In presenting the many examples of people approaching death who Sequin has cared for, a common theme emerges. Rather than a passive silence, many approaching death wish to be at home, surrounded by the noise of children — the noise of life — rather than the sobering silence of loneliness.
Both books try to dispel the hero myth, the one where the nurse or physician is never to allow the patient to lose hope. Yet hope and wishing for miracles get in the way of true discussion; it robs people of their death. Nuland confronts this reality head on when he describes how, when his brother Harvey was diagnosed with bowel cancer in 1989, he made “a series of mistakes. … I became convinced that telling my brother the absolute truth would ‘take away his only hope.’ I did exactly what I have warned others against.” Harvey was enrolled in an experimental therapy that showed initial promise but in the end increased and prolonged his anguish. Eventually, Harvey returned home to die.
These two books, and others, are a continuation of an expanding public interest in death. Certainly part of that interest can be attributed to the demographics of baby boomers. The group that first discovered drugs, free love, parenthood, the mid-life crisis and menopause has now discovered death. And along with those who want to face biological realities there will be those who desire to live beyond their biological means. Nuland writes we are currently in the vitamin era, following previous attempts to prolong life through the pseudoscience of monkey glands, mother’s milk, and, as King David tried, sleeping between two virgins. Coming soon will be expanded attempts to prolong life through the mass availability of human growth hormone, derived by genetic engineering, and gene therapy. Only “accurate knowledge of how a disease kills,” writes Nuland, “serves to free us from unnecessary terrors of what we might be fated to endure when we die. We may thus be better prepared to recognize the stations at which it is appropriate to ask for relief, or perhaps to begin contemplating whether to end the journey altogether.”
Which leads to the hotly debated topic of physician-assisted suicide and the right of rational individuals to decide how and when to end their lives. At this point the two books differ strongly. Nuland approves of Living Wills and other advanced care directives, instructing physicians what treatments to withhold in the face of terminal illness, but he strongly disapproves of physician-assisted suicide. Seguin, however, sees no distinction. Much of her book is devoted to a frank discussion of the practical advantages and limitations of such approaches.
Nuland, however, fails to come clean on the topic, when he mentions in passing that, “Like so many of my colleagues, I have more than once broken the law to ease a patient’s going, because my promise, spoken or implied, could not be kept unless I did so.” Seguin states quite clearly that many physicians have engaged in such activity, so why not create clear, legally-binding rules, as has been done in the Netherlands.
One Dutch physician who supports the new law says society needs a counterweight for the enormous technology of modern medicine. But more importantly he says, it gives the patient a chance to take leave openly of his children, his grandchildren, and others.
That openness seems crucial to further public discussion of death and dying. I still wonder what I would say to someone who is about to leave this earth on their own accord. Both books provide unique and moving insight into such conversations. Perhaps I now know what I might have said to my grandmother.
Douglas Powell is a graduate student at the University of Guelph.
Chris Koger of The Packer writes the U.S. Food and Drug Administration will be collecting romaine samples in California and Arizona for a year to test for salmonella and E. coli following several foodborne outbreaks linked to the lettuce.
The new program begins this month, according to the FDA, citing two E. coli outbreaks in 2018 linked to romaine, and another one in October that was suspected to be from the leafy green. In its notice on the surveillance program, the FDA also cited a 2012 Salmonella Newport outbreak from romaine.
“Consistent with the FDA’s mission to protect consumers, if one of the target pathogens is detected as a result of this assignment, the agency will perform whole genome sequencing of the microorganism’s DNA to determine its virulence and whether it is genetically related to isolates causing human illness,” according to the notice.
All samples will be tested before processing to allow the FDA to quickly find the point of origin, which has been problematic in recent outbreaks as public and federal health agencies traced lettuce through the supply chain. In part, traceability hurdles have led to the FDA’s New Era of Smarter Food Safety program, which tasks the industry with enhancing traceability methods and technology.
Trimmed and washed lettuce will be tested, but not fresh-cut lettuce, and no lettuce at the farm-level will be involved in the surveillance program.
Samples will be targeted at facilities and farms identified in the outbreaks starting in 2017, including wholesalers, foodservice distribution centers, and commercial cooling and cold storage facilities, according to the FDA notice.
Chinese officials believe the unidentified male became infected after handling and eating a wild hare on Nov. 5 in the Inner Mongolia, according to state news site XinhuaNet.
As a precaution, officials quarantined the people who had since come in contact with the man. None of them have exhibited fever or other symptoms of the plague, infamous for the Black Death pandemic during the Middle Ages.
Two cases of pneumonic plague, a highly contagious form of the disease, were confirmed in China by local health officials last week. The two patients, who also were from Inner Mongolia, were diagnosed in Beijing and are currently being treated for the condition in the Chaoyang District.
No epidemiological association has been found between the two cases, according to officials.
The plague is caused by Yersinia pestis — a common bacteria carried by rats, rabbits and squirrels, according to the U.S. Center for Disease Control and Prevention. Humans can contract the bubonic plague when bitten by infected fleas. Handling infected animals directly also can cause infection.
According to the department of health, the infections were identified in people who’d eaten Ready Pac Bistro Bowl Chicken Caesar Salad purchased at Sam’s Club stores in Maryland.
One person was hospitalized as a result of the E. coli O157 infection.
No deaths have been linked to it.
And there aren’t enough bagpipes and mandolins in rock.
I love Mondays in Australia because it’s Sunday in the U.S., football and hockey are on TV for background, the kid is at school when not in France, and I write (Sorenne painting in France).
Fourteen years ago, me and Chapman went on a road trip to Prince George (where Ben thought he would be eaten by bears) to Seattle, then to Manhattan, Kansas, where in the first week I met a girl, got a job, and then spinach happened.
Leafy greens are still covered in shit.
I am drowning in nostalgia, but things haven’t changed, and, as John Prine wrote, all the news just repeats itself.
Same with relationships.
Former U.S. Food and Drug Administration food safety chief, David Acheson, writes that on October 31, 2019, FDA announced a romaine lettuce E. coli O157:H7 outbreak for which the active investigation had ended and the outbreak appeared to be over. As such FDA stated there was no “current or ongoing risk to the public” and no avoidance of the produce was recommended.
Since that announcement, however, I have seen a number of articles condemning FDA and CDC. Why? Because the traceback investigation of the outbreak began in mid-September when CDC notified FDA of an illness cluster that had sickened 23 people across 12 states. So why the delay in announcing it to the public?
Despite the critical (and rather self-serving; always self-serving) stance on the “inexcusable” delay taken by a prominent foodborne illness attorney and his Food Safety “News” publication – which blasted a headline FDA “hid” the outbreak – my stance, having been an FDA official myself involved in outbreak investigations, is that the delay was practical and sensible.
Why? As FDA states right in its announcement:
When romaine lettuce was identified as the likely source, the available data indicated that the outbreak was not ongoing and romaine lettuce eaten by sick people was past its shelf life and no longer available for sale.
Even once romaine was identified as the likely cause, no common source or point of contamination was identified that could be used to further protect the public.
During the traceback investigation, the outbreak strain was not detected in any of the samples collected from farms, and there were no new cases.
Thus, neither FDA nor CDC identified any actionable information for consumers.
So, if it is not in consumers’ best interest to publicize an issue that no longer exists, why should they be driven away from a healthy food alternative? Why should unfounded unease be generated that will damage the industry, providing no benefit for consumers but ultimately impacting their pockets? There is just no upside to making an allegation without information. We’ve seen the impact on consumers and the industry when an announcement of a suspected food turns out to be incorrect; specifically “don’t eat the tomatoes” when it turned out to be jalapeno and serrano peppers. Having learned from such incidents, FDA’s approach is: If we don’t have a message that will help protect the public, then there is no message to be imparted.
So, rather than condemn FDA and CDC, I would commend them for getting the balance correct. And, perhaps, instead of any condemning, we should be working together to get the answers faster, to get outbreak data through better, faster, more efficient and coordinated traceability. Our entire system is too slow – a topic we have discussed many times in these newsletters.
I disagree.
The public and the scientific community need to be informed to prevent additional people from barfing.
I also rarely eat lettuce of any sort because it is overrated and the hygiene controls are not adequate.
Greek salad without lettuce is my fave.
Going public: Early disclosure of food risks for the benefit of public health
Mar.17
NEHA, Volume 79.7, Pages 8-14
Benjamin Chapman, Maria Sol Erdozaim, Douglas Powell
Often during an outbreak of foodborne illness, there are health officials who have data indicating that there is a risk prior to notifying the public. During the lag period between the first public health signal and some release of public information, there are decision makers who are weighing evidence with the impacts of going public. Multiple agencies and analysts have lamented that there is not a common playbook or decision tree for how public health agencies determine what information to release and when. Regularly, health authorities suggest that how and when public information is released is evaluated on a case-by-case basis without sharing the steps and criteria used to make decisions. Information provision on its own is not enough. Risk communication, to be effective and grounded in behavior theory, should provide control measure options for risk management decisions. There is no indication in the literature that consumers benefit from paternalistic protection decisions to guard against information overload. A review of the risk communication literature related to outbreaks, as well as case studies of actual incidents, are explored and a blueprint for health authorities to follow is provided.
A complaint was filed at U.S. 30 Diner on West Market Street in York and the inspector found 24 violations. The inspector found a sewage back-up in the basement piping system. One of the pipes was leaking and the facility was using duct tape as a repair. The inspector also says food employees were wearing soiled garments, and personal medication was found on a shelf with food. They say the entire food facility was extremely dirty with old food, trash, and dirt. The inspector also found a dog leash. The person in charge acknowledged that he brings his dog into the rear of the food facility, according to the report.

 One food delivery driver – whose identity is concealed – told CBSLA’s David Goldstein he’s heard drivers talk about helping themselves to your order.
One food delivery driver – whose identity is concealed – told CBSLA’s David Goldstein he’s heard drivers talk about helping themselves to your order.